Tips On How To Spot Severs Disease?
Overview
Severs disease or calcaneal apophysitis causes heel pain usually in growing children between age nine and fourteen. It occurs as a result of disturbance during the final development of the heel growth plate. During this time the achilles tendon is pulling strongly on the heel bone and this excessive force can cause inflammation and pain.
Causes
There is no specific known cause of Sever?s disease. However, there are several common factors associated with the condition including. Tight calf muscles. Pronated foot type (rolled in towards the ankle). Children who are heavier. Puberty/growth spurts. External factors, e.g. hard surfaces or poor footwear. Increase in physical activity levels.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The doctor might recommend that a child with Sever's disease perform foot and leg exercises to stretch and strengthen the leg muscles and tendons, elevate and apply ice (wrapped in a towel, not applied directly to the skin) to the injured heel for 20 minutes two or three times per day, even on days when the pain is not that bad, to help reduce swelling, use an elastic wrap or compression stocking that is designed to help decrease pain and swelling, take an over-the-counter medicine to reduce pain and swelling, such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin). Children should not be given aspirin for pain due to the risk of a very serious illness called Reye syndrome. In very severe cases, the doctor might recommend that the child wear a cast for anywhere from 2 to 12 weeks to immobilize the foot so that it can heal.
Exercise
Stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
Severs disease or calcaneal apophysitis causes heel pain usually in growing children between age nine and fourteen. It occurs as a result of disturbance during the final development of the heel growth plate. During this time the achilles tendon is pulling strongly on the heel bone and this excessive force can cause inflammation and pain.
Causes
There is no specific known cause of Sever?s disease. However, there are several common factors associated with the condition including. Tight calf muscles. Pronated foot type (rolled in towards the ankle). Children who are heavier. Puberty/growth spurts. External factors, e.g. hard surfaces or poor footwear. Increase in physical activity levels.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The doctor might recommend that a child with Sever's disease perform foot and leg exercises to stretch and strengthen the leg muscles and tendons, elevate and apply ice (wrapped in a towel, not applied directly to the skin) to the injured heel for 20 minutes two or three times per day, even on days when the pain is not that bad, to help reduce swelling, use an elastic wrap or compression stocking that is designed to help decrease pain and swelling, take an over-the-counter medicine to reduce pain and swelling, such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin). Children should not be given aspirin for pain due to the risk of a very serious illness called Reye syndrome. In very severe cases, the doctor might recommend that the child wear a cast for anywhere from 2 to 12 weeks to immobilize the foot so that it can heal.
Exercise
Stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
Posterior Tibial Tendon Dysfunction (PTTD)
Overview
For many adults, years of wear and tear on the feet can lead to a gradual and potentially debilitating collapse of the arch. However, a new treatment approach based on early surgical intervention is achieving a high rate of longterm success. Based on results of clinical studies of adults with flat feet, we now believe that reconstructive surgery in the early stages of the condition can prevent complications later on. Left untreated, the arch eventually will collapse, causing debilitating arthritis in the foot and ankle. At this end stage, surgical fusions are often required to stabilize the foot. 
Causes
Adult flatfoot typically occurs very gradually. If often develops in an obese person who already has somewhat flat feet. As the person ages, the tendons and ligaments that support the foot begin to lose their strength and elasticity.
Symptoms
Many patients with this condition have no pain or symptoms. When problems do arise, the good news is that acquired flatfoot treatment is often very effective. Initially, it will be important to rest and avoid activities that worsen the pain.
Diagnosis
Your podiatrist is very familiar with tendons that have just about had enough, and will likely be able to diagnose this condition by performing a physical exam of your foot. He or she will probably examine the area visually and by feel, will inquire about your medical history (including past pain or injuries), and may also observe your feet as you walk. You may also be asked to attempt standing on your toes. This may be done by having you lift your ?good? foot (the one without the complaining tendon) off the ground, standing only on your problem foot. (You may be instructed to place your hands against the wall to help with balance.) Then, your podiatrist will ask you to try to go up on your toes on the bad foot. If you have difficulty doing so, it may indicate a problem with your posterior tibial tendon. Some imaging technology may be used to diagnose this condition, although it?s more likely the doctor will rely primarily on a physical exam. However, he or she may order scans such as an MRI or CT scan to look at your foot?s interior, and X-rays might also be helpful in a diagnosis.
Non surgical Treatment
Nonoperative therapy for adult-acquired flatfoot is a reasonable treatment option that is likely to be beneficial for most patients. In this article, we describe the results of a retrospective cohort study that focused on nonoperative measures, including bracing, physical therapy, and anti-inflammatory medications, used to treat adult-acquired flatfoot in 64 consecutive patients. The results revealed the incidence of successful nonsurgical treatment to be 87.5% (56 of 64 patients), over the 27-month observation period. Overall, 78.12% of the patients with adult-acquired flatfoot were obese (body mass index [BMI] = 30), and 62.5% of the patients who failed nonsurgical therapy were obese; however, logistic regression failed to show that BMI was statistically significantly associated with the outcome of treatment. The use of any form of bracing was statistically significantly associated with successful nonsurgical treatment (fully adjusted OR = 19.8621, 95% CI 1.8774 to 210.134), whereas the presence of a split-tear of the tibialis posterior on magnetic resonance image scans was statistically significantly associated with failed nonsurgical treatment (fully adjusted OR = 0.016, 95% CI 0.0011 to 0.2347). The results of this investigation indicate that a systematic nonsurgical treatment approach to the treatment of the adult-acquired flatfoot deformity can be successful in most cases. 
Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
What Causes Arch Pain While Running?
Overview
Most flat feet are not painful, particularly those flat feet seen in children. In the adult acquired flatfoot, pain occurs because soft tissues (tendons and ligaments) have been torn. The deformity progresses or worsens because once the vital ligaments and posterior tibial tendon are lost, nothing can take their place to hold up the arch of the foot. The painful, progressive adult acquired flatfoot affects women four times as frequently as men. It occurs in middle to older age people with a mean age of 60 years. Most people who develop the condition already have flat feet. A change occurs in one foot where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Why this event occurs in some people (female more than male) and only in one foot remains poorly understood. Contributing factors increasing the risk of adult acquired flatfoot are diabetes, hypertension, and obesity.

Causes
Flat feet are a common condition. The condition is normal in infants and toddlers. Flat feet occur because the tissues holding the joints in the foot together (called tendons) are loose. The tissues tighten and form an arch as children grow older. This will take place by the time the child is 2 or 3 years old. Most people have normal arches by the time they are adults. However, the arch may never form in some people. Aging, injuries, or illness may harm the tendons and cause flat feet to develop in a person who has already formed arches. This type of flat foot may occur only on one side. Rarely, painful flat feet in children may be caused by a condition in which two or more of the bones in the foot grow or fuse together. This condition is called tarsal coalition.
Symptoms
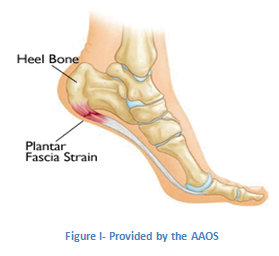
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused. If you notice that the twinges of pain you have are most commonly associated with or immediately after exercise, you might want to visit a good athletic shoe store to make sure you are wearing the right kind of shoe. Another cause of arch pain is plantar fasciitis. The plantar fascia is a tough tissue structure that holds the bottom part of the arch in place. The fascia often becomes inflamed and sore, usually as a result of repetitive motion (for example, very common in those who stand on their feet for work). The pain is often noticeable first thing in the morning and worse with activity.
Diagnosis
The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
Non Surgical Treatment
Rest is the most important thing you can do. Stay off your feet, or use a cane. Gently apply ice to the arch for at least 30 minutes, and repeat every 3 or 4 hours. Apply mild compression to the foot. Use a Fabriform PSC Foot and Ankle Strap to help support the arch, reduce swelling, and relieve pain and fatigue. This strap is easy to apply and adjust for a custom fit. Low profile allows it to fit in any shoe. Allows you to apply just the right amount of arch support/compression for your foot. Before stepping down after sleeping or resting, stretch the arch of your foot by pulling up on the ball of the foot and toes, as far as you comfortably can; hold the foot in this position for ten seconds. Repeat at least ten times. Consideration should also be given to the use of night splints. These are very effective for stretching the plantar fascia to relieve first weight bearing pain.
Surgical Treatment
In adults, the most common cause of collapse is due to the posterior tibial tendon tear. In such cases, the tendon must be repaired and a second tendon may be added to the posterior tibial tendon for strength and added support. If the foot is found to be very flat, bone realignment procedures or possible bone fusion procedures may be used to realign the foot. If the calf or Achilles tendon are found to be tight, they may be lengthened to allow better motion at the ankle and less arch strain. The forefoot may also be in a poor position and stabilization of the arch may be necessary to increase forefoot contact to the ground.
Stretching Exercises
Plantar Fasciitis stretches should always be gentle and pain free, if discomfort occurs with or after stretching decrease the intensity and duration of stretches. Stretches can usually be gradually progressed in intensity and duration over time according to individual tolerance. Plantar Fasciitis Stretch 1. Stretch for the right calf muscle (gastrocnemius) and the arch of the right foot (plantar fascia and muscles under the arches). Take your right heel close to the wall and ball of the foot upright against the wall. Move your hips forwards to the wall. Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 2. Stretch for the outside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot outwards to 2 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the left). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 3. Stretch for the inside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot inwards to 10 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the right). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 4. Stretch for the right achilles tendon and the arch of the right foot. Take your right heel close to the wall and ball of the foot upright against the wall (as for stretch 1). Move your hips forwards to the wall. Bend your right knee forwards into the wall keeping the ball of your foot upright against the wall. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times.
Most flat feet are not painful, particularly those flat feet seen in children. In the adult acquired flatfoot, pain occurs because soft tissues (tendons and ligaments) have been torn. The deformity progresses or worsens because once the vital ligaments and posterior tibial tendon are lost, nothing can take their place to hold up the arch of the foot. The painful, progressive adult acquired flatfoot affects women four times as frequently as men. It occurs in middle to older age people with a mean age of 60 years. Most people who develop the condition already have flat feet. A change occurs in one foot where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Why this event occurs in some people (female more than male) and only in one foot remains poorly understood. Contributing factors increasing the risk of adult acquired flatfoot are diabetes, hypertension, and obesity.
Causes
Flat feet are a common condition. The condition is normal in infants and toddlers. Flat feet occur because the tissues holding the joints in the foot together (called tendons) are loose. The tissues tighten and form an arch as children grow older. This will take place by the time the child is 2 or 3 years old. Most people have normal arches by the time they are adults. However, the arch may never form in some people. Aging, injuries, or illness may harm the tendons and cause flat feet to develop in a person who has already formed arches. This type of flat foot may occur only on one side. Rarely, painful flat feet in children may be caused by a condition in which two or more of the bones in the foot grow or fuse together. This condition is called tarsal coalition.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused. If you notice that the twinges of pain you have are most commonly associated with or immediately after exercise, you might want to visit a good athletic shoe store to make sure you are wearing the right kind of shoe. Another cause of arch pain is plantar fasciitis. The plantar fascia is a tough tissue structure that holds the bottom part of the arch in place. The fascia often becomes inflamed and sore, usually as a result of repetitive motion (for example, very common in those who stand on their feet for work). The pain is often noticeable first thing in the morning and worse with activity.
Diagnosis
The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
Non Surgical Treatment
Rest is the most important thing you can do. Stay off your feet, or use a cane. Gently apply ice to the arch for at least 30 minutes, and repeat every 3 or 4 hours. Apply mild compression to the foot. Use a Fabriform PSC Foot and Ankle Strap to help support the arch, reduce swelling, and relieve pain and fatigue. This strap is easy to apply and adjust for a custom fit. Low profile allows it to fit in any shoe. Allows you to apply just the right amount of arch support/compression for your foot. Before stepping down after sleeping or resting, stretch the arch of your foot by pulling up on the ball of the foot and toes, as far as you comfortably can; hold the foot in this position for ten seconds. Repeat at least ten times. Consideration should also be given to the use of night splints. These are very effective for stretching the plantar fascia to relieve first weight bearing pain.
Surgical Treatment
In adults, the most common cause of collapse is due to the posterior tibial tendon tear. In such cases, the tendon must be repaired and a second tendon may be added to the posterior tibial tendon for strength and added support. If the foot is found to be very flat, bone realignment procedures or possible bone fusion procedures may be used to realign the foot. If the calf or Achilles tendon are found to be tight, they may be lengthened to allow better motion at the ankle and less arch strain. The forefoot may also be in a poor position and stabilization of the arch may be necessary to increase forefoot contact to the ground.
Stretching Exercises
Plantar Fasciitis stretches should always be gentle and pain free, if discomfort occurs with or after stretching decrease the intensity and duration of stretches. Stretches can usually be gradually progressed in intensity and duration over time according to individual tolerance. Plantar Fasciitis Stretch 1. Stretch for the right calf muscle (gastrocnemius) and the arch of the right foot (plantar fascia and muscles under the arches). Take your right heel close to the wall and ball of the foot upright against the wall. Move your hips forwards to the wall. Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 2. Stretch for the outside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot outwards to 2 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the left). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 3. Stretch for the inside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot inwards to 10 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the right). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 4. Stretch for the right achilles tendon and the arch of the right foot. Take your right heel close to the wall and ball of the foot upright against the wall (as for stretch 1). Move your hips forwards to the wall. Bend your right knee forwards into the wall keeping the ball of your foot upright against the wall. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times.
Have I Got An Achilles Tendon Rupture
Overview  The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon. Causes Factors that may increase your risk of Achilles tendon rupture include Age. The peak age for Achilles tendon rupture is 30 to 40. Your sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Playing recreational sports. Achilles tendon injuries occur more often in sports that involve running, jumping and sudden starts and stops - such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture. Symptoms Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked. Diagnosis The diagnosis is usually made on the basis of symptoms, the history of the injury and a doctor?s examination. Non Surgical Treatment Non-operative treatment consists of placing the foot in a downward position [equinus] and providing relative immobilization of the foot in this position until the Achilles has healed. This typically involves some type of stable bracing or relative immobilization for 6 weeks, often with limited or no weight bearing. The patient can then be transitioned to a boot with a heel lift and then gradually increase their activity level within the boot. It is very important that the status of the Achilles is monitored throughout non-operative treatment. This can be done by examination or via ultrasound. If there is evidence of gapping or non-healing, surgery may need to be considered. Formal protocols have been developed to help optimize non-operative treatments and excellent results have been reported with these protocols. The focus of these treatments is to ensure that the Achilles rupture is in continuity and is healing in a satisfactory manner. The primary advantage of non-operative treatment is that without an incision in this area, there are no problems with wound healing or infection. Wound infection following Achilles tendon surgery can be a devastating complication and therefore, for many patients, non-operative treatment should be contemplated. The main disadvantage of non-operative treatment is that the recovery is probably slower. On average, the main checkpoints of recovery occur 3-4 weeks quicker with operative treatment than with non-operative treatment. In addition, the re-rupture rate appears to be higher with some non-operative treatments. Re-rupture typically occurs 8-18 months after the original injury.
The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon. Causes Factors that may increase your risk of Achilles tendon rupture include Age. The peak age for Achilles tendon rupture is 30 to 40. Your sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Playing recreational sports. Achilles tendon injuries occur more often in sports that involve running, jumping and sudden starts and stops - such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture. Symptoms Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked. Diagnosis The diagnosis is usually made on the basis of symptoms, the history of the injury and a doctor?s examination. Non Surgical Treatment Non-operative treatment consists of placing the foot in a downward position [equinus] and providing relative immobilization of the foot in this position until the Achilles has healed. This typically involves some type of stable bracing or relative immobilization for 6 weeks, often with limited or no weight bearing. The patient can then be transitioned to a boot with a heel lift and then gradually increase their activity level within the boot. It is very important that the status of the Achilles is monitored throughout non-operative treatment. This can be done by examination or via ultrasound. If there is evidence of gapping or non-healing, surgery may need to be considered. Formal protocols have been developed to help optimize non-operative treatments and excellent results have been reported with these protocols. The focus of these treatments is to ensure that the Achilles rupture is in continuity and is healing in a satisfactory manner. The primary advantage of non-operative treatment is that without an incision in this area, there are no problems with wound healing or infection. Wound infection following Achilles tendon surgery can be a devastating complication and therefore, for many patients, non-operative treatment should be contemplated. The main disadvantage of non-operative treatment is that the recovery is probably slower. On average, the main checkpoints of recovery occur 3-4 weeks quicker with operative treatment than with non-operative treatment. In addition, the re-rupture rate appears to be higher with some non-operative treatments. Re-rupture typically occurs 8-18 months after the original injury.  Surgical Treatment The best treatment for a ruptured Achilles tendon in an active individual is typically surgery. While an Achilles rupture can sometimes be treated with a cast, splint, brace, or other device that will keep your lower leg from moving, surgery provides less chance that the tendon will rupture again and offers more strength and a shorter recovery period. Surgery may be delayed for a period of a week after the rupture, to let the swelling go down. There are two types of surgery to repair a ruptured Achilles tendon and both involve the surgeon sewing the tendon back together through the incision. Open surgery, the surgeon makes a single large incision in the back of the leg. Percutaneous surgery, the surgeon makes a number of small incisions rather than one large incision. Depending on the condition of the torn tissue, the repair may be reinforced with other tendons.
Surgical Treatment The best treatment for a ruptured Achilles tendon in an active individual is typically surgery. While an Achilles rupture can sometimes be treated with a cast, splint, brace, or other device that will keep your lower leg from moving, surgery provides less chance that the tendon will rupture again and offers more strength and a shorter recovery period. Surgery may be delayed for a period of a week after the rupture, to let the swelling go down. There are two types of surgery to repair a ruptured Achilles tendon and both involve the surgeon sewing the tendon back together through the incision. Open surgery, the surgeon makes a single large incision in the back of the leg. Percutaneous surgery, the surgeon makes a number of small incisions rather than one large incision. Depending on the condition of the torn tissue, the repair may be reinforced with other tendons.